


A COVID Success Story
The Uttar Pradesh Story

In the second half of March of 2021, the new Delta Variant of COVID exploded in the Northern Indian State of Uttar Pradesh, rocketing from 151 new cases on March 15th to 37,994 new cases on April 24th. Hospitals were overwhelmed, and many predicted cases would continue to double relentlessly week after week until all of Uttar Pradesh was infected.
That’s not what happened. In fact, eight weeks later, daily cases had fallen by more than 99%. Over the past six months, Uttar Pradesh has seen a 99.9% reduction in daily new cases. Their most recent COVID seven-day averages were nine cases and one death. (For comparison, Canada’s most recent seven day averages were 2,419 daily cases and 27 deaths.)
In graph form, it’s quite spectacular:
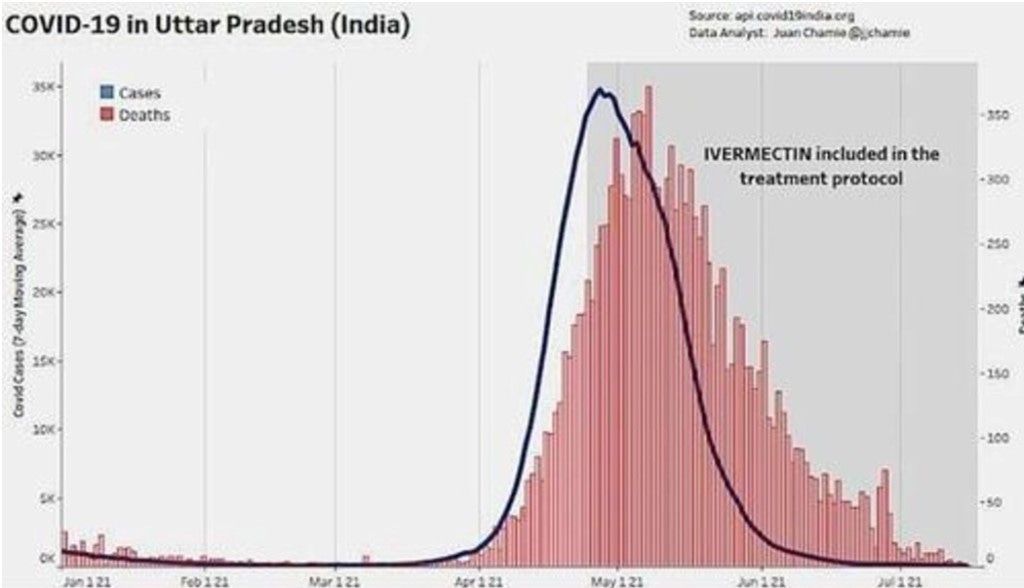
How was it possible that a poor, largely-unvaccinated Indian State of 225 million people was able to rein in an extremely infectious new variant so quickly and so successfully?
Here’s what Uttar Pradesh did. When COVID infections skyrocketed, they quickly trained up 140,000 two-person teams of lay-people to go house-to-house, and village to village. Anyone suspected of having COVID was given a rapid-response COVID test.
Anyone who tested positive for COVID was given a kit containing the following items:
1) A pulse oximeter and a digital thermometer.
2) N95 Masks.
3) Tablets of paracetamol, Vitamin C, Vitamin D, and a Multivitamin with Zinc.
4) Doxycycline tablets.
5) Ivermectin tablets for both the patient and their immediate family.
The lay health teams provided instruction on how to use the materials in the kit, as well as ongoing follow-up.
Why did they do what they did? They used huge numbers of lay people for their outreach teams because that was the only way to test and treat millions of people in a matter of weeks. They used rapid response tests because it meant they could treat people immediately, in the field. An occasional false-positive test result was considered worth the huge increase in speed that rapid response testing provided.
Oximeters were easy for patients to use. Stick a finger in the oximeter and a digital readout told the percentage of oxygen in the blood. Above a certain percentage, the patient was instructed to stay at home and get plenty of rest. Below that percentage – go to the hospital.
Masks for all family members reduced the odds of other family members getting infected.
Vitamins C, D, and Zinc were part of the kits because they had been shown in various studies to reduce the severity of COVID symptoms.
A not-infrequent complication of COVID is bacterial pneumonia. Giving everyone infected with COVID a prophylactic dose of the antibiotic doxycycline was done to try to reduce the chances a COVID infection would be made worse by the added complication of bacterial pneumonia.
The inclusion of ivermectin in the kits may shock Canadians, but India has conducted numerous clinical trials of ivermectin, and ivermectin had been routinely used as both a COVID prophylactic and an early treatment medication for more than a year in Uttar Pradesh.
We don’t know exactly why rates of COVID have fallen so precipitously in Uttar Pradesh. They are testing 200,000 people a day, so it was not a lack of testing. It appears extremely unlikely there have been sufficient COVID cases for Uttar Pradesh to have achieved herd immunity. We also know Uttar Pradesh has seen a far greater reduction in cases than neighbouring Indian States with differing anti-COVID strategies. What is undeniable is that Uttar Pradesh has been spectacularly successful in reducing cases of the Delta Variant. Clearly they’ve been doing something right. If nothing else, what has happened there deserves more attention and investigation.
I think what has happened in Uttar Pradesh is very exciting and incredibly important. It mystifies me that this story has received so little media coverage in North America. It also disturbs me.
I suspect this article is the first time most readers will have heard about the successes in Uttar Pradesh. Why is this so? I suspect it is because the mainstream media now considers it a duty of responsible journalists to ‘protect’ us from any information which might cause us to doubt or question what Canadians have been told we must do to end the COVID pandemic.
In this case, I feel mainstream journalism has been ‘protecting’ us from crucial information that gives us the opportunity to question and re-think everything we think we know about how to end this pandemic. For months we have been told if we can just get vaccination rates a little higher, the pandemic will soon be over. That hasn’t happened. Instead, cases numbers of COVID in Canada remain at high levels and our ICU’s are struggling to cope.
There’s also good evidence from other jurisdictions that vaccines alone are not sufficient to stop the spread of COVID. More than 91% of Ireland is now fully vaccinated, but this week Ireland saw its highest rate of COVID hospitalizations in seven months:
Perhaps the time has come to examine more closely what other jurisdictions have done to combat COVID. In saying this, I am not trying to dispute or deny the importance of vaccination, only to address the on-the-ground reality that vaccination alone has not brought the COVID pandemic to a close in Canada.
Bruce O’Hara
Author’s Note: In the past, I’ve had very good success in getting various op-ed pieces published in major Canadian newspapers. But more than a dozen Canadian newspapers turned this one down. I don’t believe the problem is with the quality of my writing, but that the content challenges the status quo narrative about how we need to deal with this pandemic. It definitely qualifies as news non grata!
Sources:
Information on the number of COVID cases in the period from March through June comes from the John Hopkins University. Do a google search on the key words “COVID Stats Uttar Pradesh” and it shows up the first item. Case numbers by date can be read off the graph. Do the same for “COVID Stats Canada.”
Information on what Uttar Pradesh did can be found at:
The WHO reports on the number of teams in Uttar Pradesh here:
Dr John Campbell has gathered considerable information on what was done in Uttar Pradesh, with sources:
Uttar Pradesh’s use of ivermectin finally made it into the mainstream press in this MSN piece:
Some of the history of ivermectin use in Uttar Pradesh is given here:
following article contained excellent information, slightly weakened by the fact that the md doing the reporting feels compelled to use a pseudonym.
Current information on vaccination rates and population in Uttar Pradesh are here:
https://www.covid19india.org/state/UP
Information that ivermectin was given to family members of those testing positive for COVID in Uttar Pradesh is presented about halfway through this video interview with Dr. Pierre Kory. Cory is the founder of flccc.net – a support organization for Front Line COVID Critical Care providers in the US.
s now a huge body of research on ivermectin. Ivermectin is one of WHO’s Essential Medicines – for humans. In almost fifty years of use, and almost 4 billion doses, it has shown an excellent safety profile. Though ivermectin is most often used as an anti-parasite, it has previously also been used as an antiviral to treat HIV-1, Dengue Fever and Zika Virus. There best compilation of the research evidence in support of ivermectin can be found at:
Here’s an excellent summary of the controversy surrounding ivermectin, including a summary of the research that supports ivermectin.
https://www.zerohedge.com/covid-19/never-say-neigh-fda-lists-horse-drug-approved-covid-treatment