

Reclaiming the Ethical Principles of Individualized Medicine
One-size-fits-all medicine is ethically challenged - and bad medicine!


Three cornerstone principles of individualized medical care have been tossed aside during the COVID pandemic:
1) Respect for each individual’s unique health needs.
Individualized medicine is both an ethical principle and a pragmatic precept.
The pragmatic part comes from the recognition that making treatment plans based on the particular strengths, needs, vulnerabilities and history of each patient generates better health outcomes.
It’s why most North Americans have a family doctor, and why that doctor typically takes a detailed medical history during their first session with a new patient - so that your medical care is tailored to fit your specific, individual needs.
2) Medical Autonomy
Individualized medicine puts the patient in charge. It is the patient, not the doctor who must live with the consequences of any medical treatment the patient receives. Therefore, the patient must be the final arbiter of whatever medical treatment they receive, even if those decisions run contrary to the advice of their physician. (Jehovah’s Witnesses have the right to refuse blood transfusions, for example.)
3) All Medical Altruism Must Be Voluntary
In the past, if a person lost both their kidneys in a car accident it was perfectly acceptable for the patient’s surgeon to beg and cajole relatives to donate a kidney. If the same surgeon sought a court order forcing a relative to donate a kidney, that would have been seen as an obvious violation of the would-be donor’s rights.
While public health officials were free to offer incentives to encourage the public to donate blood, forcing people to donate blood was considered to be unethical - even when blood supplies were at critical levels. Even with a medical procedure as innocuous as giving blood, the moral edge was that medicine could ask altruism of people, but not force it upon them.
In the past, even medical personnel were accorded the right to choose to be altruistic - or not. Though a health administrator was permitted to encourage - perhaps even badger - medical personnel to get the most current flu vaccine, there was a general consensus within medicine that it would be ethically improper to make taking the seasonal flu vaccine a prerequisite for continued employment.
Prior to the COVID pandemic, most public health policy was based on non-binding recommendations, and/or one or other form of information bulletin, press release, or advice to doctors. The assumption was that you didn’t have to force people to behave in ways that would reduce their risk of dying; an instinct for self-preservation would lead most of us to follow public health guidelines which were well-argued and evidence-based.
Occasionally, public health policies were given legal backing. Many jurisdictions required doctors to report every time they diagnosed a sexually-transmitted disease, for example. But the law was used sparingly to enforce public health policies prior to COVID.
This use of non-binding strictures had two advantages. First, it supported the ethical right of the individual to be the final arbiter of their own healthcare. Secondly, it also left individuals free to modify or ignore public health recommendations that were inappropriate to their own health needs. It was strongly supportive of individualized medicine, in other words.
These pre-existing norms were completely overturned during the COVID pandemic. The extent to which health authorities relied on public health edicts, legal coercion and one-size-fits-all health proscriptions during the COVID pandemic was unprecedented in modern times.
We were told there was no choice, that the COVID pandemic was a such a huge health emergency that it required a draconian response.
But there was a choice.
North America’s mainstream media has painted Sweden as being terribly negligent in its response to COVID, insinuating that Sweden passively allowed COVID to run rampant in Sweden.
In fact, Sweden handled the COVID pandemic exactly how all previous disease pandemics had been handled by public health authorities pretty much everywhere prior to COVID.
They quarantined the sick. They made public health recommendations. They issued information bulletins letting people know who was at highest risk, and how individuals could best reduce their personal risk of infection.
It’s not as though Swedes didn’t change their behaviour during the pandemic. The difference was that Sweden didn’t impose a one-size-fits-all straitjacket on their population.
Sweden trusted that, given good advice, ordinary Swedes would modify their behaviour appropriately. They didn’t need to be forced to make good health decisions.
The failure of lockdowns is not specific to America. The following bar graph looks at cumulative excess deaths over the three years of the pandemic in each of the OECD nations:
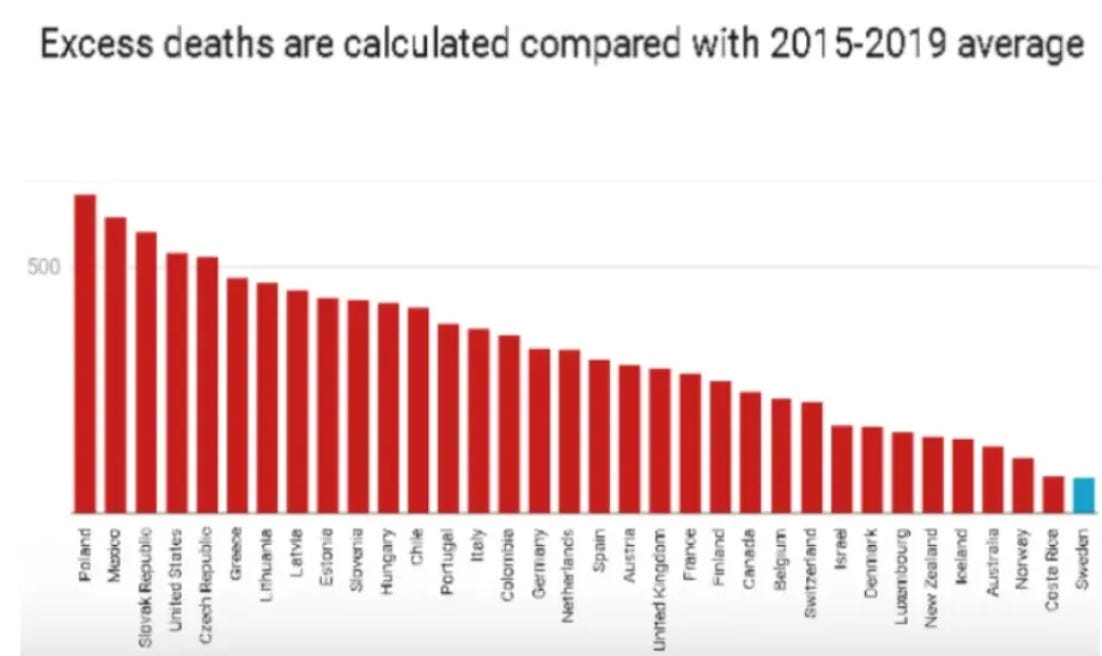
Do you see that short blue bar on the right? That’s Sweden, with the lowest rate of excess deaths of any of the 34 OECD countries. The other 33 countries in the OECD all imposed lockdowns, and every single one of them had a higher rate of excess deaths than lockdown-free Sweden. Lockdowns failed to save lives everywhere they were used.
A second arena where all three of these ethical principles were abandoned during the COVID pandemic was in the attempt to force everyone to get vaccinated.
Authorities ignored the principle of individualized treatment by demanding that those who already possessed natural immunity still needed to get vaccinated.
For all previous vaccines, each person was considered to have the ethical right to decide whether to get vaccinated or not. Even medical personnel. Not so for COVID vaccines.
Suddenly it was not only ethically-permissible to coerce people into getting vaccinated by threatening to take away their livelihood, it was now ethically mandatory that everyone get vaccinated to supposedly protect granny.
What was so different about the COVID pandemic that it required the overnight abandonment of principles which had been ethical cornerstones for decades?
COVID is, at best, only marginally more deadly than the common flu for people under the age of 65. If smallpox, tuberculosis, polio, AIDs, SARS, and Ebola were not sufficient grounds to set aside the core ethical principles of individualized medicine, what possible justification was there for setting them aside for COVID?
It’s pretty clear to me these longstanding principles of individualized medicine were not abandoned after any concerted and careful consideration. As with the principle of informed consent, they were tossed aside in a wild-eyed panic, a panic triggered by some spectacularly bad forecasting of how deadly COVID might prove to be.
We cannot allow the blind panic of North America’s public health officials to rob us of these cornerstone principles of medical ethics. We must reclaim what has been taken from us.
PS: My apologies to anyone who already got this post via Wholistic. I often post on topics that aren’t of interest to Stephanie, so I suspect half or more of my posts here on NewsNonGrata in the future will only be here.
I’m also tempted to make a separate, different post for my own readers when I do write something for Stephanie, and just link to her post in a postscript - as I did on Friday.
Apropos to that idea, a post of mine on her site that I originally didn’t post here is Whatever Happened to the Principle of Informed Consent, which makes a good book-end to the above post. I’ve since posted it here.
Bruce, This is as terse and well-articulated a piece on this overwhelmingly important topic as I have seen. Kudos.
In the current edition of The Economist (available at Save-on-Foods) I see an article on the excess deaths across the world.